Periodontal Surgery

4-6 weeks after scaling and root planing, periodontal re-evaluation is performed: full mouth periodontal probing and charting is completed at this visit. Areas of the mouth that have higher residual probing depths, bleeding, and radiographic bone loss, will require surgical treatment.

1. Ensure that the root surfaces of the teeth are clean of bacteria by directly visualizing root and bone interface – this is the primary goal of periodontal surgery.
Figure 1 – The green zone demarcates “effectiveness” of scaling & root planing – this depth can be thoroughly cleaned without surgery. Pockets deeper than 3.5mm (red zone), cannot be adequately accessed using non-surgical methods. Periodontal surgery is recommended to thoroughly clean this depth.
2. Address/treat the bone loss. Bone loss results in irregular topography, which is shaped and contoured to allow the gum tissue to lay lower on the tooth (osseous surgery), and/or bone grafting is performed to regenerate lost tooth support (guided tissue regeneration utilizing bone graft, membrane barrier, growth factors).
3. Facilitate patient hygiene by enabling access to the root surfaces of the diseased teeth. This is accomplished by decreasing probing depth by osseous surgery and/or bone grafting. Proper hygiene is key in long term periodontal stability and treatment of gum disease!!!
There are three general categories of periodontal surgery in treatment of periodontal disease – gingivectomy, osseous surgery, periodontal regeneration.
Gingivectomy

Severe gingival overgrowth secondary to the patient’s medications (calcium channel
blocker used to treat high blood pressure).
Pocket depths ranged from 6-12 mm, making it impossible for the patient to adequately access and clean.
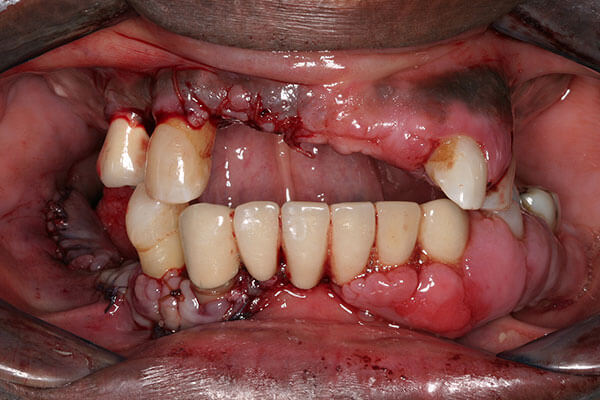
In gingivectomy procedures, excess gum tissue is removed. Note the reduced tissue size (pocket depth) and improved tissue tone. The patient is now able to access and clean his teeth
Osseus Surgery

Case #1 – Presurgical condition. The patient is probing 9mm
pocket depths between the upper molar teeth.

6 weeks following osseous surgery – the molars are now probing a healthy 3 mm. The patient is now able to access and clean more effectively around and between the molar teeth.

Case #2 – Osseous surgery on the lower left was completed 2 mos prior – probing depths are all within normal limits. Patient can now access and clean root surfaces, thereby maintaining their periodontal condition.
Periodontal Regeneration

Case #1 – Severe bone loss lower molar with furcation involvement. Previous dentist recommended extraction. Periodontal regeneration was performed using bone graft with a resorbable barrier membrane.

2 year follow-up shows complete regeneration in furcation. Patient has been compliant with good hygiene and regular recall visits.

Case #2 – Severe bone loss on maxillary molar. Periodontal regeneration surgery performed using bone graft mixed with protein growth factor.

Almost 100% regeneration noted 2.5 years later! Plus, she received two dental implants!